
The Specificity of Words & Nerves | 4
What the nervous system reveals about sensation, language & communication:

Meaningful communication is an absolute drive for human beings, one for which we have evolved a uniquely sophisticated capacity to produce language.
We develop our familiarity with patterns of linguistic structure so fluently within life however, that we may inevitably come to take this capacity for granted.
Human language is as much a process of information input as it is output. It requires sensory afference (neural conduction towards the brain) in the first instance, such as visual, auditory or tactile stimulation, followed by cognition in the second.
The synthesis of language requires a variety of discrete anatomical systems to perform across the human lifespan. These are presided over by the neural coordination of the brain, and the pulmonary (of respiration) anatomies, which are mainly the lungs, the pleura surrounding the lung, the rib cage surrounding this, and the diaphragm inferior to these.
Collectively these structures provide airflow for the laryngeal and orofacial structures to influence through dynamic changes to the potential space (the space which can occur within structures) of the larynx and oral cavity in order to produce an array of precise sounds. Via these structures, a fluid coordination occurs between the information we receive and the information we convey.
Linguistic cognition hinges on our comprehension of phonetic, lexical, grammatical, syntactic and semantic patterns. In this way, we can understand the layers of human communication as a living and breathing endeavour, made up of linguistic patterns, anatomical structures and physical forces acting in elegant coordination with one another.
The ease and utility of communication which language provides us, and the comprehension of meaningful language that our senses and nervous tissues mediate, have gradually become the cornerstone of human civilisation. We can easily make the case perhaps, that language is human civilisation, for nothing that is humanly societal, communal or familial, can exist without this simple and yet detailed means of communication we understand as our language.
The result of cumulative human experience, language is for us all an inheritance of a wider heritage and yet also an individuated art.

Consider the lexicography of Egyptian hieroglyphs, which communicate meaning through a language of symbolic imagery. When compared to the letters and numbers of today, to us they seem quite conspicuous, for the alphabets of many modern languages, those languages still ‘alive’ and in use today, are not pictographic, albeit they contain a residual pictography that has become part of a convention of lexical symbols. We can take Chinese calligraphy to be an example.
The alphabet used in English, is instead an organised set of simpler patterns which we seldom consider to have symbolic meaning individually. They have become such a standardised unit of symbol, that what individual meaning they had in signifying something beyond their phonetic sound has become secondary if not trivial.
In our early years of life, we consider these symbols to be devoid of any meaning other than what they are agreed to mean in order for a language to function. With time we discover that the combination of letters provides for their expansion into words and sentences. Years later, we utilise vocabulary or turn of phrase, and through these there come intonations, with subtle verbal and vocal cues nestling into their rise and fall. All told, these symbols which allow us to infer and relate patterns of sound become the providence of our communicable thoughts and feelings, and through them, our humanity is mediated.
We do not utilise the entirety of our linguistic heritage, because there is an economy of meaning to life. It is neither desirable nor practical to incorporate the whole vocabulary of English language into our communications, it does not allow us to achieve the purposeful aims of everyday life, despite it having the largest vocabulary of any language on Earth. The crux of human language lies in the purpose of the communications we make. The purposeful selection of words in any given language made by any individual using it is a fraction of those available. Language has the potential to frustrate when used to obscure on the one hand, or to imbue life with meaningful communication, musicality and poetry on the other. The right word in the right place then, allows us to specify that the sum words available to the speaker can be called the lexicon of their language.
Lexical selection is the remit of the neurolinguistic comprehension and interpretation of the words recorded within the mind; selection is also however, dependent on the context in which these words are to be used, and also on the intent of the user. Crucial aspects of language may change with the individual’s intent, and the context in which the candidate word is to be applied by the person in their use of language.
All neurolinguistic functions combine in order to aid the selection of words during the life history of a human being. Even in infancy when we babble, the production of sound in and of itself is essential, as it aids our refinement of crude sounds into shaped sounds, known as phonemes, which are then combined into words. This process is entirely dependent on coordination of the orofacial, laryngeal and respiratory musculatures and their neural innervation.
Sound we at first only hear, yet then come to associate with aspects of the physical world, and finally, to imbue the information we sense with coherent meaning. We develop deep a bonding affection with our mother’s heart beat en utero, for example, and sense the world more and more as we develop.
Without these crucial neurolinguistic functions, a multitude of words may be at our disposal, but not necessarily put to use in a way that represents reality, or otherwise, concepts that are relatable by human beings to one another.
In light of patterns we perceive in our environment, or from written language, we learn to recognise the world around us as perceptibly separate from ourselves, and to describe its features and effects on us.
The electrical and chemical patterns which signal within our bodies to coordinate our living functions and responses, including that of writing and speaking, are well observed in clinical evidence and neuroanatomy. This is the principle function of science, to observe without imposition.
Neurolinguistic and anatomical sciences are not the means through which we should understand ourselves, but they can help us to understand aspects of ourselves and of our nature which are confusing or intriguing; for instance, by offering insight into how and why the selection of words in order to convey information is so effective at converting real world patterns we sense through the nervous system, we understand that the electrochemical patterns in our neural tissues can be affected by factors beyond our control and by choices we make on a day to day basis. We can understand the nature of a neurological disorder, and suspend the judgement which as human beings with mechanistic fears and beliefs, we might otherwise be predisposed to.
These electrochemical patterns we sense are transduced (converted from a physical force into a codified neural pattern) then into information that can be interpreted by the brain, which may then be expressed by linguistic information within the networks of that organ. Sometimes we might not say, ‘Ow!’, when we are exposed to physical pain; and instead, ‘Agh!’, or with the emphatic disinhibition of adulthood, ‘F#£k!’, will suffice; - yet the word, Ow!, still forms a very early part of any English speakers vocabulary.
The neurally mediated process of language is, in its entirety, why specific words serve us so well when used with the precision of both verbal and written communication. Conversely then, if there is a loss of neural function due to an injury or disease which affects the temporoparietal or temporofrontal brain tissues (introduced in the 3rd article of this series), is significant enough, the individual would likely suffer a loss of linguistic functionality, including the recall of words.
Which words however, and in what manner the symptoms present, makes for the crucial distinction between which of the functional neurolinguistic tissues are being affected, and how best a clinical intervention can restore these functions.
SPACE, TIME & CLINICAL HISTORY of the LINGUISTIC BRAIN:
The process of learning a language requires the construction of new connections, represented spatially within the brain regions responsible for language and memory.
Linguistic patterns are made up of words, formed of verbs, subjects and objects; their meaning must be made available to conscious working memory in order for them to be compared and contrasted with those previously acquired. This is linguistic fluency in a nutshell.
By way of converse example, if we hear or read a language we do not understand, we have no prior record of the sounds or written words with which to compare, and thus to decodify their meaning.
The brain parenchyma - a useful anatomical word derived from the ancient Greek which means, ‘an infusion of that within which differs from that without’, admittedly gets somewhat lost in direct translation. Here we need only understand that this word specifies the functional tissue of an organ, as distinct from its supporting or connective tissues.
Within the parenchyma of the brain, we find the microstructure of neuronal networks establishes a vast array of functions that go well beyond the sum of their number, and in the case of language learning, that there is a relationship between physical space and time.
The spatial retention and processing of language within the brain has been revealed to some degree by contemporary neuroscientific research, in that a second language learned later than the first is situated in an adjacent space. Whereas the more simultaneously two languages are learned, the more spatially proximate their processing becomes within the microcosm of networked connections in the brain which are dedicated to language and memory.
This illustrates again than the neuroanatomy of language is the result of a functional space that is stimulated by iterations of sensory experience.
To briefly reiterate, linguistic function is the result of sensation, cognition and affect; patterns of language become information because they are derived directly from auditory and visual sensations of the world, or from descriptions related by human beings to one another through language. Both of these activities require a synchronous and fluid continuity between neural comprehension and interpretation, which can be influenced by thoughts and emotion.
For example, we can understand what a specific word means, but not be able to successfully interpret its meaning in a specific context. We can likewise initially sense something in the world, and then our senses can organise this into information for transmission to the brain, but both these steps precede the cerebral level of organisation which allow us to comprehend and interpret the information. In other words, the information is not intelligible by virtue of sensation in and of itself.
Hence, the loss of one or more of our linguistic functions, i.e., of comprehension or interpretation during states of neurological disease, has offered medical practitioners and clinical anatomists opportunities to demarcate the neuroanatomical structures and connections responsible.
The first cerebral localisation of function is attributed to Thomas Willis in the 17th century; as an anatomist and physician he coined the term neurology, and attributed localised function to the cerebral cortex for the first time. Recall that ‘cortex’ means tree-bark, and is the outermost and most major layer of the brain.
Through the post-mortem dissection of individuals who had experienced a loss of speech function in life, the localisation of language to a specific part of the brain was demonstrated by Pierre-Paul Broca in the 19th century. In such cases Broca discovered a left frontal lobe lesion had induced a set of symptoms that were pre-emptively termed by him in 1861 as ‘aphemia’.
This term is now more readily differentiated from the term aphasia and its sub-classifications, where aphemia denotes a neurological speech dysfunction in which the ability to articulate ideas is lost, despite the capacity to comprehend and produce speech through coordination of the bucco-facial musculature being retained.
The buccinator muscle, derived from the Latin for trumpeter, is crucial to shaping the potential space within the oral cavity such that blowing air into wind instruments and whistling are possible.
The word buccal means ‘cheek’, a square bilateral muscle which forms part of the lower face; it is an accessory to the muscles of mastication when it aids the formation of a food bolus, from the ancient Greek meaning a ‘clod’ of soft material, until the bolus is liquified and compacted enough for it to be swallowed from the oral cavity into the oesophagus. The buccal muscle happens also to be utilised in certain orofacial expressions.
The musculo-facial process of verbal expression is clinically termed, arthria, where respectively partial or complete loss of this function is termed, dys-arthria and an-arthria, where each prefix of, dys-, means ‘reduced’, and that of, an-, means ‘without’. Arthria is itself derived from the same root as articulacy and articulate, meaning to utter in distinct parts, but simultaneously from, compose, attach or separate by joints, whether the adjective or verb form of the word is being used.
We see that the language of anatomy is itself an elegant composition of forms that can be used to describe the elegant composition of forms. It is a language which has the potential to be used artfully when describing features and functions of the human form in life, and in specifying the loss of those functions in a meaningful way. Being able to use language to make these distinctions in a meaningful way, means that the functions are represented accurately by the language used to describe them, and that the partial or complete loss of them can be differentiated or compared.
The word root of arthria is interesting in relation to further derivations from its root. In fact this word and its clinical counterparts have other distant relatives which we include more often in everyday language, including alarm, article, armour, order, harmony, artist and arm - all derived from an indo-European root word, ar, which became their prefix, and means simply - to fit together. Thought and art can be understood principally as ways of fitting things together.
Broca also observed the effects of the brain lesions he investigated, and attempted to fit together how these symptoms might indicate a physical source of linguistic processing. He articulated his hypothesis through cogent and precise language. In doing so, he ultimately contributed to humanity’s understanding of ourselves as a highly expressive species in a wider continuum of life.
The loss of speech function observed by Broca and others was sometimes coincident with right-side hemiplegia, a complete paralysis of the side of the body which is contralateral to the damaged somatomotor area of the brain, where the functions that are local to the precentral gyrus discussed in article 3 are processed by its cortical grey matter.
This hemiplegia occurs in the event that pathways of the middle and front of the brain, known anatomically as the left parietal and frontal lobes, are damaged. If this damage includes Broca’s area, then the somatomotor cortex may also be affected.
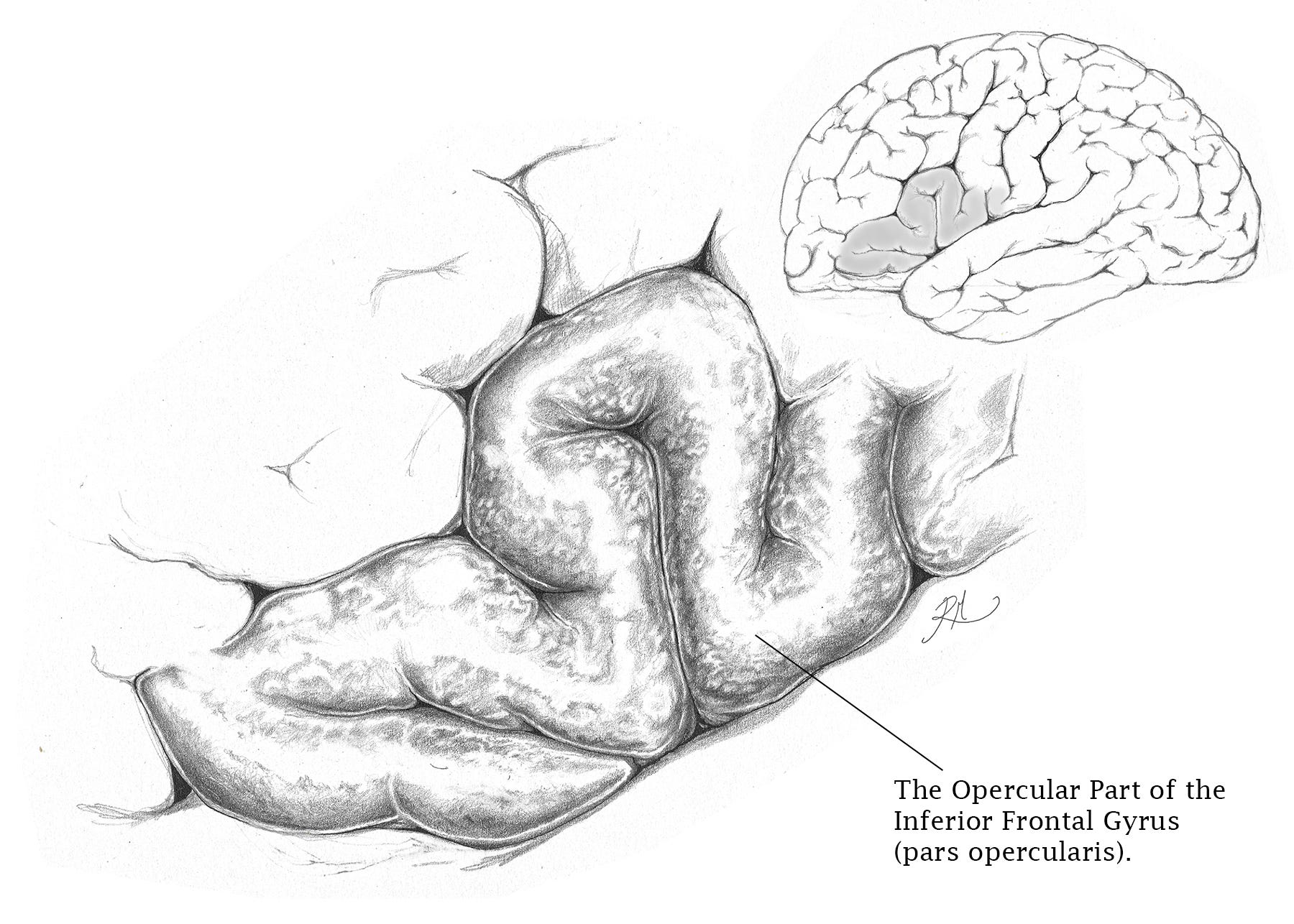
This is simply because the opercular part of the inferior frontal gyrus that contributes to Broca’s area, abuts the precentral gyrus, and in doing so forms the lower third of the precentral sulcus.
It is the opercular part to which our ability to recognise tone of voice in our spoken native language is attributed.
Due to the decussation (crossing-over) of somatomotor efferent fibres from the left brain hemisphere to the contralateral side of the body, the patient under the same effects that Broca initially observed presents with a loss of speech function and right side paralysis.
Once again, the neuroanatomical specificity of terms is crucial. The loss of function is attributable to the 1st order neuron because the patient presents with a loss of speech and right side hemiplegia, with no peripheral injury to 2nd order neurons of the paralysed side (see article 2 in this series for an explanation of 1st and 2nd order neurons).
This paralysis is defined neuroanatomically as a central plegia because the 1st order (in this case the upper) motor neuron is affected. This diagnostic term is in contrast to a peripheral plegia, wherein the 2nd order neuron is affected, and paralysis is being caused outside of the central nervous system.
A case of partial denervation is termed hemiparesis, rather than hemiplegia, where the word denervation itself means the loss of nerve function without a qualifying cause.
A secondary influence on the spinal plexi (from the latin pletere, meaning ‘of plaited structure/pattern’) may occur in cases of peripheral plegia.
This results from partial or complete denervation of the cervical, brachial, thoracic, lumber or sacral outflow of nerve plexi, where ‘outflow’ denotes how these nerves diverge from the spinal cord to form the main branches of the peripheral nervous system.
The cauda equina for example, the ‘horses tail’, is that outflow of nerves which innervate the pelvic region and the lower limb.
We will explore in the next article how meaningful differences between the presentation of linguistic ability and understanding come to inform diagnoses made by clinicians and inferences made by scientists.
Thank you for reading!