
The Specificity of Words & Nerves | 2
What the nervous system reveals about sensation, language & communication:

Sensation precedes language:
By exploring examples of neural sensation, and the way in which our senses confer information about the world to us, not only can we explore how language is shaped before it is even uttered or written, we can also explore why human language and the neurosensory system are reflections of each other. In order to function, sensation and language must differentiate the reality of events and stimuli from one another in this way…
We know a human being is exposed to a wide variety of internal and external stimuli and physiological changes throughout a 24 hour period, and across a lifetime; our response to many of these changes requires us to be aware of them, on one level or another.
At the human scale, the world is especially complex, thus, our neural capacities allow us to meet the challenges of what we create, by observing their effect with assiduous measure, adjusting our designs or actions accordingly.
Our functional neuroanatomy reflects this demand by its delineation into afferent and efferent transmission. This means respectively, those signals issued from more distal locations to the brain (sensation), and in the converse direction, those signals which operate from the brain to innervate the action of more distal (motoric) tissues such as muscles and glands.
The spinal tracts which mediate all somatic (muscle, skin) and visceral (organs/glands) as sensations from the body to the brain for example, subserve the brain by transmitting afferent signals electrochemically, from the most peripheral to the most central neurons.
These nerve fibres are referred to as 1st order and 2nd order neurons, where respectively they define the first and second neuronal cells which synapse in the chain of transmission. This description of a stepwise process differs however, from the terms upper and lower motor neurons. These terms denote neurons which descend (efferently) from the brain to the spinal cord when upper motor neurons, and to complement this outflow, neurons which proceed from the spinal cord to the target musculature or organ are termed lower motor neurons. Lower motor neuron disease is then, a disease of the peripheral nervous system, affecting nerve fibres beyond the central nervous system, outside of the spinal cord.
The terms 1st, 2nd and 3rd order neurons, are useful, simply because they reflect the functional neuroanatomy of both afferent and efferent transmission. Our initial aim is to understand the specification of which order neuron operates during its functional role, and how it may be affected by injury or disease, and through which tissues each neuron travels, and how a loss in their function would present outwardly. This requires the use of specific terms, especially when the neural tissues in question are part of a branching complex, and this is almost always the case…
The trigeminal nerve, meaning the ‘threefold’ nerve, for example, issues general sensation from its 3 branches, which approximate to the upper, middle and lower face. For example then, symptoms of neuralgic pain in the temporomandibular junction, (where the jaw hinges to the the skull), indicate the mandibular branch of the trigeminal nerve is being affected. Whereas symptoms of headache would suggest the ophthalmic branch of the nerve, which innervates sensation to the forehead, eyes and midline of the nose, is the branch of concern.
Being able to distinguish the intrinsic structure of the trigeminal nerve through language is incredibly useful. But what about specifying different orders of neuron in relation to neurological dysfunction, what do the words actually provide us with here? We can use an example which deviates from afferent sensation momentarily to illustrate this by drawing on the efferent functions of the facial nerve.
Presentations of stroke must be differentiated from facial (Bell’s) palsy. An underlying understanding of which order of neuron and which branch of the cranial nerve in question is affected is clinically crucial, even though the facial signs may be sufficient to posit a diagnosis.
In terms of the muscles of facial expression which indicate these signs, by either losing or retaining their contractile innervation, these nerve branches function to confer muscle tone and contraction (and not sensation), therefore we ask which of 1. the upper (1st order) or lower (2nd order) motor neurons that descend from the somatomotor cortex have been affected, and 2. which subsequent subnuclear branch of the facial nerve is affected; - for it is these nerves which underly the neuroanatomical structures delineating a stroke from facial palsy. This is specifically because the 7th cranial nerve, the facial nerve, innervates the muscles of facial expression via 2 efferent neurons that synapse within its nucleus (the facial nucleus).
The diagnosis hinges anatomically on the synapsing of these 2nd order neurons where they proceed from the aptly named, pons verolli - i.e. ‘bridge of Verolli’ region of the brainstem, shortened usually to, the pons, and in which the facial nucleus is located, yet also where connections between the medulla and cerebellum are made.
There are some specific terms here that help us delineate the connections and their states: first is the antonym of innervation, which is denervation, that denotes a loss of electrochemical activity in the nerve; second is the word ipsilateral, which in the context of brain hemispheres denotes the same side of the brain which has been damaged; finally their is contralateral, which is the antonym of ipsilateral, and simply means the adjacent hemisphere, which in this context has not been affected by damage. The potential space between them is the medial longitudinal fissure.
In the scenario of stroke or facial palsy, the stroke presents outwardly as a loss of tone in the muscles which the lower facial nerve innervates, hence the cheek and mouth sag. If the affected neuron is 2nd order from the facial nucleus, becoming the lower facial nerve branch, then the forehead is spared due to a backup nerve being available. This compensatory nerve is a 1st order neuron which also descends from the contralateral somatomotor cortex to synapse in the pons.
This nerve compensates for denervation of the somatomotor nerve affected in the ipsilateral hemisphere by maintaining innervation of the lower facial nerve branches; if however, both 2nd order neurons are affected, then complete denervation of the facial nerve will occur, presenting as paralysis (palsy) of one half the face (as seen in the facial presentation of 1) and an inability to wrinkle the forehead.
The precision of these terms is elementary prima for any neurologist or keen neuroanatomist, because the wiring and the factors at play when denervation occurs, require knowledge of the underlying structures. This language must go beyond the interpretation of symptoms alone; especially when research on this mechanism is being conducted, communicated, or in the event that either the patient’s condition worsens despite intervention, or presents with more than one type of neural problem.
How then do we infer the specific direction in which a 1st order neuron is transmitting its signal, whether toward or away from the brain, when compared to higher 2nd or 3rd orders which synapse in the brain?
A 1st order neuron is afferent when stimulated at a free nerve ending under the skin, and its transmission is directed towards the brain. Conversely, a 1st order neuron that descends from the brain to innervate a muscle say, courses towards that tissue in order to transmit efferently. Efferent nerves descend, afferents ascend.
An afferent transmission from the skin via the 1st order will subsequently synapse with a 2nd order neuron that transmits its signal up the spinal cord. This ascending fibre can be specified as an afferent post-synaptic neuron, as it is situated within the spinal cord, and is a functional structure in a 3 step process, ending in a 3rd (order) neuron of the brain.
Ascending via the brainstem into the thalamus, the 2nd order neuron then synapses with a complex of modular nuclei (bundled synapses which represent functional units) before projecting via the 3rd order neuron into the higher order cortical tissues that receive specific somatosensory stimuli.
Somatosensory afferent transmissions are issued from more peripheral locations via the spinal cord.
Where the term, viscera, is used to denote organ tissues, rather than somatic tissue, the word soma means ‘of the body’. Soma is in some way an etymological offshoot of the ancient Greek word demas, meaning ‘of the living body’; - a fact which may indicate that the majority of anatomical classifications made by early modern scientists were the result of observing cadavers more often than living patients, yet showing also how the specificity of a word’s meaning can develop over time.
The term ‘somatosensory cortex’ denotes an area of cortical brain tissue which processes afferent sensations from somatic tissues. It is the complement of the motoric efferent processing which is provided by the adjacent somatomotor area of cortical tissue, that is precentral to the sulcus dividing each. The term ‘precentral gyrus’, denotes the anatomical relation of the somatomotor area to the central sulcus (of Rolando). The sulcus divides these two functional areas, as seen in the image below.
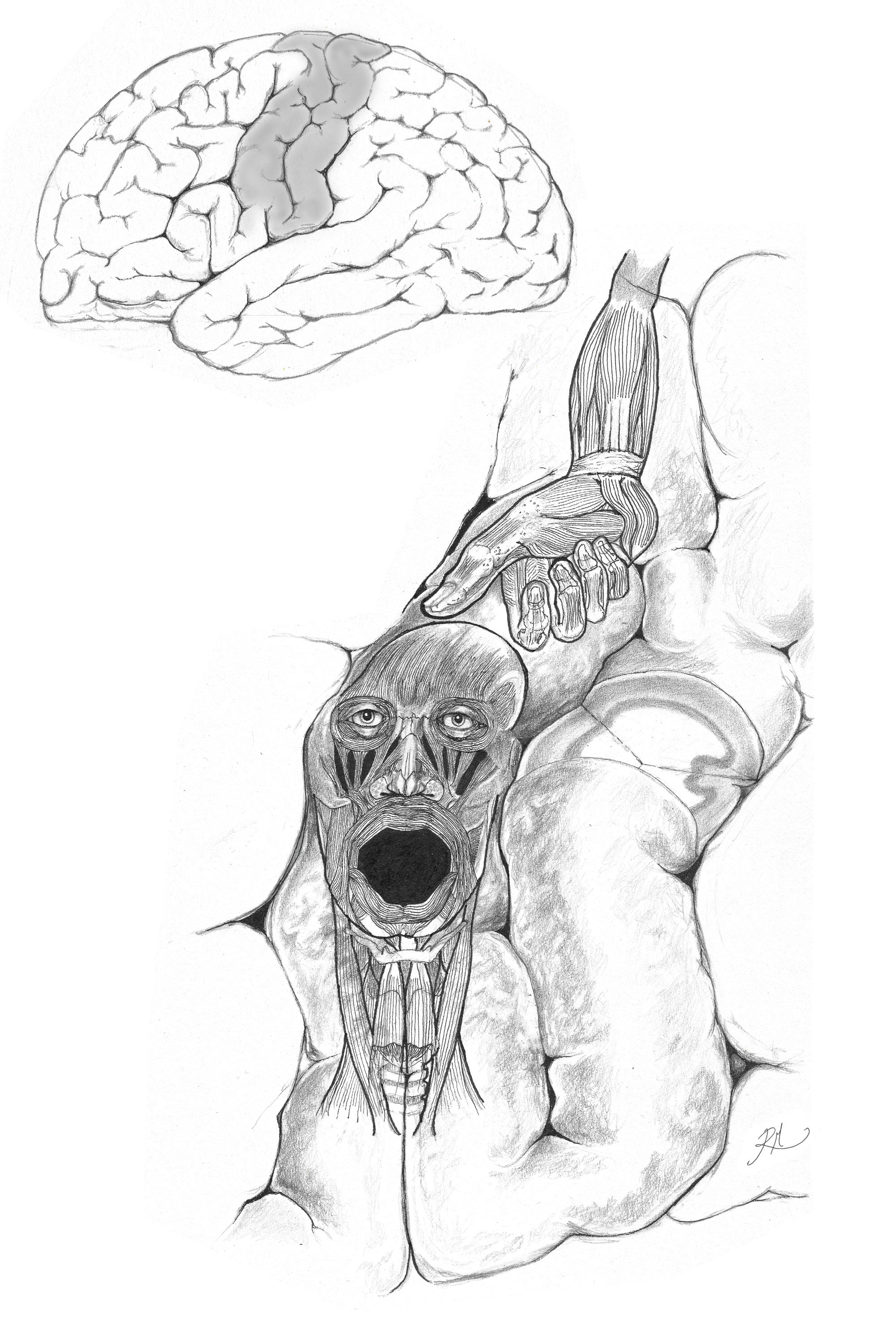
The somatomotor cortex dedicates a disproportionate area to the articulation of the mouth, lips and tongue through the descending nerve tracts. The situation of the tongue is not in the same area of the cortex as the mouth, hence its absence in the above image.
Fibres which descend from the inferior 3rd of the somatomotor cortex (precentral gyrus) originate from the laryngeal and orofacial motor cortices therein, and innervate these lower facial muscles.
These efferent fibres terminate as 1st order neurons in the cerebral peduncles of the ventral midbrain, found within the brainstem. In brainstem nuclei which include the facial and trigeminal nuclei mentioned earlier, these descending fibres synapse with 2nd order neurons that contribute to the fine motoric control of speech. The course of these fibres collectively form the corticobulbar tract. Everything here is distinguishable in terms of locale and the flow of electric transmission. But with regards to language…
…the disproportionate representation of the orofacial musculature in the somatomotor cortex, evidently reflects how important linguistic precision is for our species. The production of speech requires the inclusion of the laryngeal complex (which is represented in the inferior 1/3rd of the somatomotor area, as above), and also requires the respiratory system in order to coordinate the passage of air necessary for vocalisation and phonation, which alongside the orofacial musculature, demands the precise coordination of more than 100 distinct muscles, 1/6th of those in the entire human anatomy.
Although each term, gyrus and cortex, may be used synonymously to denote this area of the parietal lobe of the brain, they have distinct meanings. The term ‘somatosensory cortex’, denotes the functional aspect of the cortical tissue; but the term ‘postcentral gyrus’ allows the area to be identified and located as a raised area of tissue when observing the exterior surface of the brain topographically.
The fact that this is the surface and not volume of a tissue, can be easily termed as a, pial surface. This parenchymal surface of the brain lies deep to the arachnoid mater that overlays the brain and allows for cerebrospinal fluid to be circulated. The specificity of how brain regions and areas relate to each other is built into the nomenclature so as to convey information, and in distinguishing each form and their positional relations, helps us to comprehend these complex structures more easily and yet also more completely.
A useful takeaway here is that it pays not to avoid using specific terms when they describe something complex, or assume such terms are synonymous because they at face value describe the same thing. It is absolutely valuable to describe the simplest structures at their initial levels of detail, as in the hemispheres of the brain being divided into two, symmetrical and connected via the corpus collosum. But the more complex the structure is, the more specific the communication of its form and function need be.
Similarly, the term postcentral, obviously implying ‘posterior to the centre’, is used because the anterior-posterior axis clarifies the reference points for orientation of the brain in the cranial vault of the skull, whereas the word ‘behind’ does not specify anatomical orientation or relation. ‘Behind’ what?
As human beings, we sense the physical composition of our world through neural tissues, each relying on their own physical composition in order to confer function.
As established, the synapsing of 1st through to 3rd (and even 4th) order neurons, mediates the electrochemical transmission between body and brain, allowing the brain to process information that is afferently sensed within as well as without.
Worth noting is that there are 8 ascending spinal tracts, and 4 descending, which at least by number indicates there are twice as many ascending tracts, which are dedicated to transmitting sensation as afferent information towards the brain, than there are descending tracts dedicated to the efferent control of movement. We can to some degree infer then, that the nervous system assigns twice as much of its functionality to receiving information from the body and outside world as it does to movement. This has much to do with the dual imperative for us to move only when we have information which allows us to safely do so, and to issue close control over visceral and somatic functions via the autonomic nervous system.
For instance, the afferent spinal tracts known as the dorsal columnar medial lemniscal, and in partnership with them, the spinothalamic tracts, respectively mediate the sensation of both stereognostic (tactile detail) and crude forms of touch, with each transmitting the signal issued from integumentary (skin) nerves that detect an object held in the hand.
Like all anatomical labels, these nerve tracts are named to denote certain notable features, such as their shape, as in ‘columnar’, their position as in ‘dorsal’, and their course as being ‘spino-thalamic’, ascending through the spine and into the thalamus.
The dorsal columnar medial lemniscal pathway is so named because it is situated in the posterior half of the spinal cord, but on reaching the brainstem it decussates to the medial lemniscal tract.
The phylogeny of this tract (its evolutionary history) is relatively more novel in its evolution than the spinothalamic tract. It is responsible for our sense of fine touch, vibration (save for the head), conscious proprioception, and stereognostic touch - which discriminates complex objects, allowing us to identify them by prehensile (grasp) use of our hands, but without necessarily having to look at the object.
The hand is a prehensile limb, that is by definition, ‘able to grasp’, and through which we can palpate, in order to sense the shape of an object with greater or lesser sensitivity.
Because the spinothalamic tract is far older than that of the dorsal columnar tract, it indicates that our evolutionary ancestors developed crude touch before that of the stereognosis which heavily contributes to the recognition of an object through touch alone.
Neuroanatomical mechanisms such as these are fundamentally how the sensation informing what we experience is mediated, to then directly inform what we describe of our sensory experience through language.
The tracts mediating the sensation of an object at hand in specialised degrees of detail; yet this process alone, as mediated by the spinal tracts specified above, does not allow us to successfully interpret what the object is, nor whether the object is of any value. This would require a range of modalities, including both comprehension and interpretation, each the remit of executive decision making in the brain itself.
In the next article, we shall explore the language making process as it proceeds from that of sensation.